Children with Stevens-Johnson syndrome associated with Mycoplasma pneumoniae were more likely to develop pneumonia, to have fewer affected skin sites, and to have respiratory symptoms prior to the condition, a study found.
“The spectrum of M. pneumoniae–-associated Stevens-Johnson syndrome disease was consistent with previous reports, including severe mucositis and milder skin manifestations,” reported Dr. Daniel Olson of the University of Colorado, Aurora, and his associates (Pediatrics 2015 July 27 [doi:10.1542/peds.2015-0278]).
 Courtesy Wikimedia Commons/Rottem et al./Creative Commons License
Courtesy Wikimedia Commons/Rottem et al./Creative Commons License
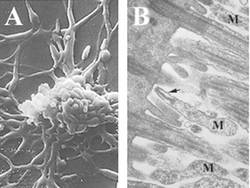
Image A shows filamentous M. pneumonia. Image B shows M. pneumonia (M) attached by the terminal tip organelle (arrow) to ciliated mucosal cells.
In the largest reported pediatric outbreak of Stevens-Johnson syndrome at Children’s Hospital Colorado, from Sept. 1 to Nov. 30, 2013, eight children met the criteria for the condition, median age 11.5, including five boys. Five were PCR positive for M. pneumoniae, all were susceptible to macrolides, and three had clinical symptoms indicating M. pneumoniae was likely. All five positive cases had radiographic pneumonia, and none had been exposed to medication. All eight children received azithromycin, and all were discharged well.
Following the outbreak, the researchers identified all hospitalized SJS cases back to October 2008 and classified them as likely or unlikely to be associated with M. pneumoniae, based on a positive PCR result or positive M. pneumoniae immunoglobulin.
Compared with the 23 cases not associated with M. pneumoniae, the 17 that were associated with the bacteria had 10 times greater odds of radiographic pneumonia. Those associated with M. pneumoniae also had 30 times greater odds of having preceding respiratory symptoms, had 22.8 greater odds of having an erythrocyte sedimentation rate of at least 35 mg/dL, and had 4.5 greater odds of less than three skin sites affected.
“Subjectively, the physicians caring for hospitalized Stevens-Johnson syndrome patients reported less severe skin disease and more severe mucositis, including ocular disease, among the M. pneumoniae–associated Stevens-Johnson syndrome group,” the authors reported. Those with and without M. pneumoniae infection had similar hospitalization durations, treatments, ICU admissions, and ocular amniotic membrane grafting.
“We offer two likely explanations for the recent outbreak,” the authors wrote. “Our initial hypothesis was that a new M. pneumoniae strain with a greater predisposition to induce Stevens-Johnson syndrome was circulating in the community. A second, more likely hypothesis is that there was a large outbreak of M. pneumoniae in the community, which resulted in an increased rate of Stevens-Johnson syndrome due to an overall increased rate of exposure to M. pneumoniae.”
In future M. pneumoniae–associated outbreaks of Stevens-Johnson syndrome, the authors recommend collecting respiratory samples and evaluating treatments.
The National Institutes of Health funded the research. Dr. Glodé is a member of a Pfizer data safety monitoring board for an unrelated vaccine, and Dr. Robinson served on a one-day scientific advisory board regarding Biofire’s gastroenteritis pathogen polymerase chain reaction panel. (Biofire markets a respiratory pathogen panel that was used to detect the M. pneumoniae infections in this study.)